
Outcomes of Differentiated Thyroid Cancer Patients Treated with Surgery and Radioactive Iodine at SQCCCRC
Abstract
Objective
To evaluate the treatment outcomes of patients with Differentiated thyroid cancer (DTC) who underwent total thyroidectomy followed by RAI therapy at the Sultan Qaboos Comprehensive Cancer Care and Research Centre (SQCCCRC) in Oman.
Methods
This is a retrospective observational clinical study conducted at SQCCCRC. The study included all patients diagnosed with DTC who were admitted to SQCCCRC between June 2021 and November 2023. A total of 255 patients were identified and met the inclusion criteria for this study.
Results
The mean age at diagnosis was 39.9 ± 12.4 years (range: 14–79), with 78% of patients being female.
The mean BMI was 30.3 ± 6.4 kg/m², with nearly half of the cohort (48.2%) classified as obese (BMI ≥ 30). Most patients had papillary thyroid carcinoma (92.9%), while follicular and Hürthle cell carcinoma accounted for 5.9% and 0.8% of cases, respectively.
Based on the American Joint Committee on Cancer (AJCC) staging, 86.3% of the patients were classified as stage I and 3.9% as stage II. Six patients (2.4%) had stage IVB disease. According to American Thyroid Association (ATA) risk stratification the majority were low-risk. Patient age was strongly associated with disease stage. The distribution of metastatic cases varied by region, with the highest proportion observed in Dhofar. Most patients (87.1%) received a single dose of radioactive iodine (RAI), with a median cumulative dose of 3.7 mCi). At six months post-treatment, 70.2% of patients had a TG level < 0.2 ng/mL.
Conclusion
The outcome of therapy in majority of our patients is favorable with 72% having excellent biochemical response at last follow up. None of the patients with distant metastasis achieved excellent response and a high proportion of them came from the Dhofar governorate, a targeted intervention would be of benefit.
Low risk patients require special attention and may need radioactive iodine during follow up, unlike other regions and hence warrant very close follow up and further review to establish the best practice guidelines in our region.
Article Information
- Received
- Accepted
- Published
Academic Editor: Anubha Bajaj, Consultant Histopathologist, A.B. Diagnostics, Delhi, India
Checked for plagiarism: Yes
Review by: Single-blind
Copyright © 2026 Omayma Elshafie, et al.
 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Corresponding author: Omayma Elshafie, Department of Endocrinology, Sultan Qaboos Comprehensive Cancer Care and Research Centre (SQCCCRC), University Medical City, Sultanate of Oman —
Competing Interests
The authors have declared that no competing interests exist.
Funding
No specific funding statement was provided by the authors.
Data Availability
No data-availability statement was provided by the authors.
Acknowledgements
We thank the head and neck surgeons and multidisciplinary teams involved in the care of these patients, including Dr Yahya Al Baadai and Dr Laila Al Masoudi (SQUH head and neck surgeons), Dr Khalil Makki (AFH head and neck surgeon ), Dr. Sharjeel Usmani and Dr Anjali Jain (Nuclear Medine Consultants), Medical Physics , pathology, anesthesia, and nursing teams at SQUH and SQCCCRC
Citation:
Introduction
Thyroid cancer is the most common endocrine malignancy worldwide. Among all cancer types, thyroid cancer has the ninth highest incidence rate worldwide 1. It is responsible for more than 586,000 cancer diagnoses and 43,000 deaths every year. In Oman, thyroid cancer is the second leading cause of cancer in the overall Omani population and among Omani women 2, 3, 4, 5. The incidence of thyroid cancer is increasing globally 6. Increasing thyroid cancer incidence in Oman has also been observed in the most recent years 3. Number of thyroid cancer diagnoses in the Omani population increased from 173 cases in 2018 to 235 cases in 2019 5.
Thyroid cancer is divided into differentiated, medullary, and anaplastic subtypes based on pathology. Differentiated thyroid cancer (DTC) has a good prognosis, but distant metastasis may lead to death due to progression of disease 6. The treatment for metastatic DTC consists mainly of surgery, radioactive iodine (RAI) therapy, thyroid-stimulating hormone (TSH) suppression therapy, and rarely external beam radiotherapy 7.
Thyroidectomy is the definite and main treatment option of thyroid cancer 9, 10, 11, 12. Limited research has been done on the outcomes of thyroid cancer in the Omani population. A single study in Oman had reported that 83% of differentiated thyroid cancer patients were disease-free at their final follow-up 13. Kunjumohamed et al reported that lymph node metastasis, angio-vascular invasion, widely invasive follicular thyroid carcinoma, and number of lymph nodes involved were associated with worse prognosis in this population.
More research is needed to measure the outcomes of thyroid cancer after treatment in the Omani population. In this study, we aim to investigate the outcomes of thyroidectomy used with radioactive iodine for the treatment of DTC at the SQCCCRC. We examined the effect of demographical and clinical factors on the patients’ outcomes.
Aim of the Study
This is a retrospective observational study to examine the outcomes of thyroid cancer treated by surgery and radioactive iodine at the SQCCCRC. The study examines the effect of age, sex, body mass index, region, histopathology (tumor type and TNM status (primary tumor (T), regional lymph node (N), and distant metastasis (M) stage), iodine dose, baseline and follow up stimulated and unstimulated thyroglobulin Tg), thyroglobulin antibody (TgAb), and stimulated and unstimulated thyroid-stimulating hormone (TSH) levels), lymph node metastasis and distant metastasis on the patients’ outcomes.
Methods
Study Design
This is a retrospective observational clinical study conducted at the Sultan Qaboos Comprehensive Cancer Care and Research Centre (SQCCCRC). The study aimed to evaluate the treatment outcomes of patients with DTC who underwent total thyroidectomy followed by RAI therapy.
Study Population
The study included all patients diagnosed with DTC who were admitted to SQCCCRC between June 2021 and November 2023.
Inclusion Criteria
· Histologically confirmed diagnosis of DTC (including all subtypes).
· Underwent total thyroidectomy as primary treatment.
· Received RAI therapy.
· Age ≥ 13 years at time of diagnosis
Exclusion Criteria
· Incomplete clinical records or missing follow-up data.
· Patients with medullary or anaplastic thyroid cancer subtypes.
· Patients who did not receive both surgery and RAI.
Data Collection
Demographic and clinical data were extracted from the hospital's electronic medical records. Collected variables were included:
Demographics: age, sex, region of residence, body mass index (BMI).
Clinical and pathological data: tumor histology, TNM staging (T: tumor size, N: lymph node involvement, M: distant metastasis), type of surgery, RAI dose.
Biochemical markers: pre- and post-treatment levels of stimulated and unstimulated thyroglobulin (Tg), thyroglobulin antibody (TgAb), and thyroid-stimulating hormone (TSH)
Disease status: presence or absence of local or distant metastasis, and recurrence status (new vs recurrent tumor).
Outcomes
The primary outcome is the biochemical response to treatment, defined as a stimulated Tg < 1 ng/mL or suppressed Tg < 0.2 ng/mL at either 6 months or 12 months following RAI therapy.
The secondary outcome is the presence of metastasis, categorized as:
Local persistence: residual thyroid tissue or cervical lymph node involvement detected by neck ultrasound 6 months post-treatment
Distant metastasis: identified through diagnostic whole-body I-131 scan and/or cross-sectional imaging (CT and PET/CT), as clinically indicated
Statistical Analysis
Descriptive statistics were used to summarize patient characteristics: medians and interquartile ranges for continuous variables, and frequencies and percentages for categorical variables. Associations between demographic/clinical variables and the primary outcome (biochemical response) were analyzed using Chi-square tests and logistic regression models. A multivariate logistic regression was performed to identify independent predictors of treatment response, adjusting for potential confounders. A p-value < 0.05 was considered statistically significant.
Sample Size Analysis
A total of 255 patients met the inclusion criteria and were included in the analysis. Categorical variables and treatment response frequencies were compared between clinically and demographically defined subgroups, including lymph node involvement, administered radioactive iodine dose, and baseline thyroglobulin levels. All statistical tests were two sided, and a p value of ≤0.05 was considered statistically significant. Fisher’s exact test was used for comparisons of proportions. Continuous variables were summarized using descriptive statistics and compared between groups using the twosample ttest.
All statistical analyses were performed using R software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria) and Stat version 19.0 BE (StataCorp, College Station, TX, USA).
Results
Baseline demographic and tumor characteristics
A total of 255 patients diagnosed with DTC were included in the study. The mean age at diagnosis was 39.9 ± 12.4 years (range: 14–79), with 78% of patients being female. Geographically, the majority were from the Batinah (34.9%) and Muscat (21.8%) regions, with a small percentage from other governorates or outside Oman.
The mean BMI was 30.3 ± 6.4 kg/m², with nearly half of the cohort (48.2%) classified as obese (BMI ≥ 30). Most patients had papillary thyroid carcinoma (93.3%), while follicular and Hürthle cell carcinoma accounted for 5.9% and 0.8% of cases, respectively.
Tumor size at diagnosis was less than 2 cm in 80.5% of patients, and the median maximum tumor diameter was 2 cm (IQR: 1.2–3 cm). Lymph node involvement (N1) was reported in 37.9% of cases, whereas in 31.5% of the cohort the LN status was unknown or Nx. Distant metastases were documented in 5.5% of patients. Features associated with more aggressive disease, including extrathyroidal extension and angio-vascular invasion, were present in 11.1% and 32.8% of patients, respectively. Multifocal disease was observed in 58.7%.
Based on the American Joint Committee on Cancer (AJCC) staging, 91.7% of the patients were classified as stage I and 4.2% as stage II. Six patients (2.5%) had stage IVB disease. According to American Thyroid Association (ATA) risk stratification, 49.8% were low-risk, 40% intermediate-risk, and 10.2% high-risk. The median duration of follow-up was 14 months (IQR: 12–24), ranging from 1 month to over 21 years. Demographic characteristics of the study cohort are presented in Table 1, Figure 1.
Table 1. Demographic and tumor characteristics.| Demographic Characteristics | Mean ± SD or n (%) (unless defined otherwise) |
| Age, years (range) | 39.9 ± 12.4 (14–79) |
| Sex | |
| Male | 56 (22) |
| Female | 199 (78) |
| Region | |
| Muscat | 55 (21.8) |
| Dhofar | 23 (9.1) |
| Dakhiliyah | 37 (14.7) |
| Batinah | 88 (34.9) |
| Sharqiyah | 26 (10.3) |
| Dhahirah | 14 (5.6) |
| Other (Wusta, Musandam, Buraymi) | 3 (1.2) |
| Non-Omani | 6 (2.4) |
| Missing | 2 |
| BMI, kg/m² (range) | 30.3 ± 6.4 (15.9–49.7) |
| <18.5 (underweight) | 5 (2) |
| 18.5–24.9 (healthy) | 50 (19.8) |
| 25–29.9 (overweight) | 75 (29.6) |
| ≥30 (obese) | 123 (48.6) |
| Missing | 2 |
| Histological subtype | |
| Papillary | 237 (93.3) |
| Follicular | 15 (5.9) |
| Hurthle cell | 2 (0.8) |
| Missing | 1 |
| Tumor size in cm | |
| <1 cm | 124 (52.8) |
| 1–1.9 cm | 65 (27.7) |
| 2–3.9 cm | 38 (16.2) |
| ≥4 cm | 8 (3.4) |
| Largest tumor size (cm), median (IQR) (range) | 2 (1.2–3) (0.1–9.5) |
| Lymph node status | |
| N0 | 72 (30.6) |
| N1 (N1a, N1b, unknown) | 89 (37.9) (40, 39, 10) |
| Nx | 74 (31.5) |
| Missing | 20 |
| Distant metastases present | |
| Yes | 13 (5.5) |
| No | 224 (94.5) |
| Missing | 18 |
| Extrathyroidal extension | |
| Yes | 26 (11.1) |
| No | 209 (88.9) |
| Missing | 20 |
| Angio-vascular invasion | |
| Yes | 77 (32.8) |
| No | 158 (67.2) |
| Missing | 20 |
| Tumor focality | |
| Unifocal | 97 (41.3) |
| Multifocal | 138 (58.7) |
| Missing | 20 |
| AJCC prognostic stage | |
| I | 220 (91.7) |
| II | 10 (4.2) |
| III | 2 (0.8) |
| IVA | 2 (0.8) |
| IVB | 6 (2.5) |
| Missing | 15 |
| ATA risk category | |
| Low | 117 (49.8) |
| Intermediate | 94 (40) |
| High | 24 (10.2) |
| Missing | 20 |
| Duration of follow-up (months), median (IQR) (range) | 14 (12–24) (1 month–21 years) |
Figure 1. Region distribution of the study population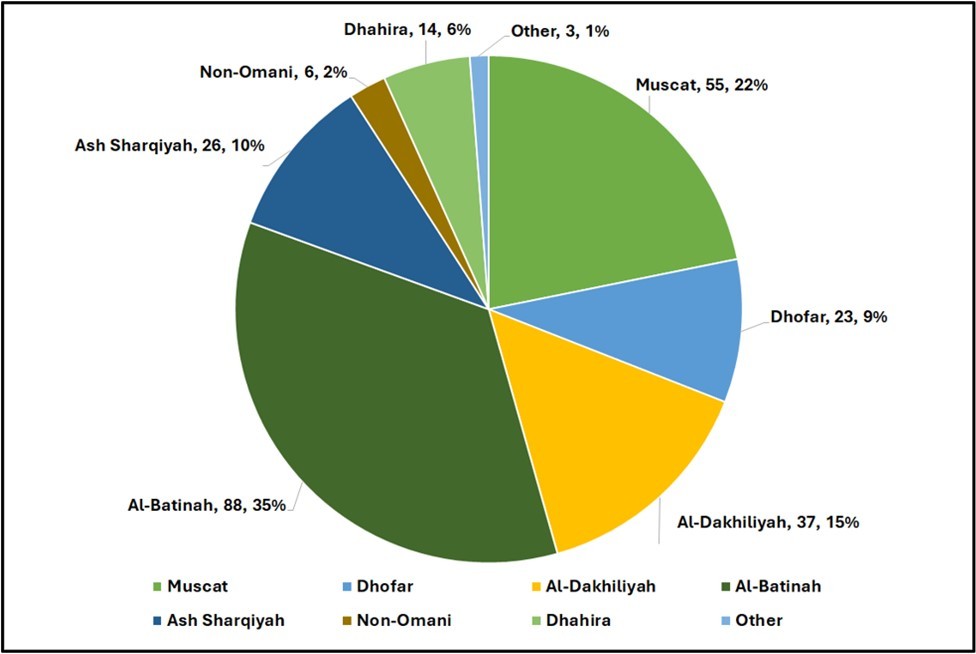
Download figure
Association of Patient Demographics with Disease Characteristics
Patient age was strongly associated with disease stage (Table 2). Among patients younger than 45 years, the vast majority (98.8%) were classified as AJCC Stage I, with only 2 patients (1.2%) having Stage II disease and none with Stage III or IV. In contrast, older patients (≥45 years) exhibited a broader distribution of stages: 75% were Stage I, while the remaining 25% were diagnosed with Stage II–IV disease. This difference was statistically significant (p < 0.001, Fisher’s exact test). This relationship remained significant when age was analyzed as a continuous variable. Patients with Stage I disease had a significantly lower mean age compared to those with Stage II–IV disease (38.2 ± 10.3 vs. 57.1 ± 15.9 years, respectively; p < 0.001, two-sample t-test). No significant associations were observed between sex and disease stage in our cohort (p=.857). While the overall association between BMI and AJCC stage did not reach statistical significance (p = 0.059), a more focused analysis revealed a significant relationship between high BMI and advanced disease. Specifically, all patients with Stage IV disease had a BMI ≥30, and this association was statistically significant (p = 0.006).
The distribution of metastatic cases varied by region (Table 3), with the highest proportion observed in Dhofar, accounting for 5 cases (38%) of all metastases. Other regions with notable proportions included Muscat and Al Batinah (2 cases; 15% each), followed by Al Dakhiliyah, Ash Sharqiyah, Non-Omani patients (1 case each). Statistical analysis showed a strong association between Dhofar region and the presence of distant metastasis (p = 0.003) (Figure 2).
Table 2. AJCC stage by age group.| AJCC Stage | Age <45 (%) | Age ≥45 (%) | Total |
| Stage 1 | 163 (76.2) | 51 (23.8) | 214 |
| Stage 2 | 2 (20) | 8 (80) | 10 |
| Stage 3 | 0 (0) | 2 (100) | 2 |
| Stage 4 | 0 (0) | 7 (100) | 7 |
| Total | 165 (70.8) | 68 (29.2) | 233 |
| Region | Number of metastatic cases (%) |
| Muscat | 2 (16.7) |
| Dhofar | 5 (41.7) |
| Al-Dakhiliyah | 1 (8.3) |
| Al-Batinah | 2 (16.7) |
| Ash Sharqiyah | 1 (8.3) |
| Non-Omani | 1 (8.3) |
| Missing | 1 (8) |
Figure 2. Proportion of metastatic disease by region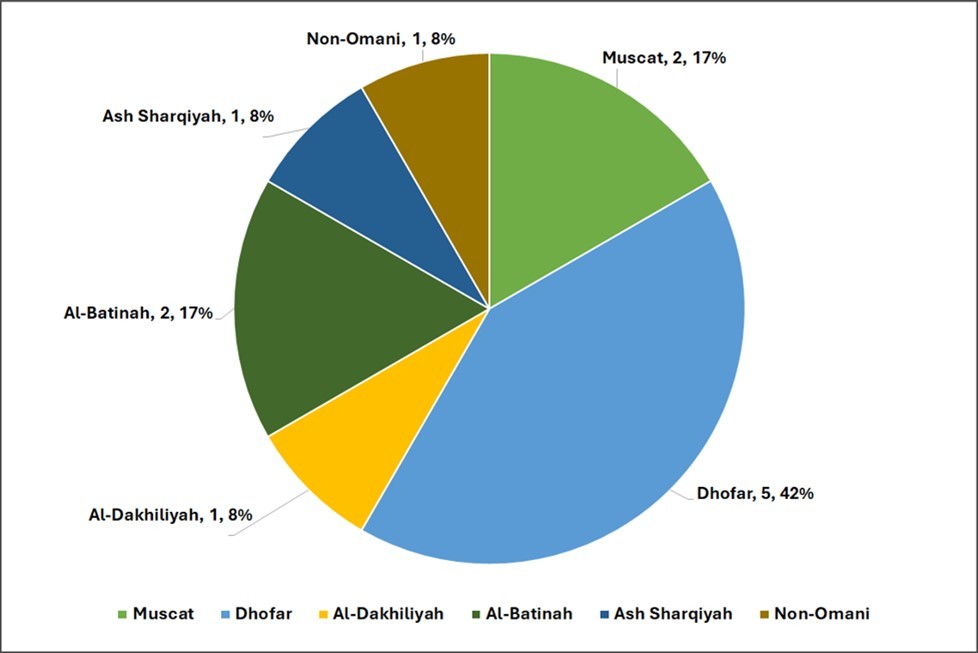
Download figure
Biochemical profile at baseline
At postoperative baseline, 43.2% of patients were biochemically hypothyroid (TSH > 4.3 mU/L). Median stimulated TSH was 100 mU/L (IQR: 75.7–100). The median thyroglobulin (TG) level was 0.6 ng/mL (IQR: 0.07–4.0), with 34.1% having TG < 0.2 ng/mL. Similarly, median stimulated TG was < 1ng/mL is 32.6% of the patients. Both suppressed and stimulated anti-thyroglobulin antibodies (TG-Abs) were negative (< 115 IU/mL) in 87.3% and 84.6% of cases. (Table 4)
Table 4. Baseline and TSH-stimulated thyroid cancer biomarkers in the study cohort| Biomarker | Median (IQR) or n (%) (unless defined otherwise) |
|---|---|
| TSH ( mU /L) | 3 (0.30–13) |
| ≤ 0.5 (Hyperthyroid) | 72 (28.2) |
| 0.51–4.30 (Euthyroid) | 73 (28.6) |
| > 4.30 (Hypothyroid) | 110 (43.2) |
| Stimulated TSH ( mU /L) | 100 (75.7–100) |
| > 4.30 (Hypothyroid) | 255 (99.6) |
| TG (ng/mL) | 0.6 (0.07–4) |
| < 0.2 | 87 (34.1) |
| ≥ 0.2 | 168 (65.9) |
| Stimulated TG (ng/mL) | 2.56 (0.45–11.79) |
| < 1 | 83 (34) |
| ≥ 1 | 161 (66) |
| Missing | 11 |
| TG ABS (IU/mL) | 18 (15–48) |
| < 115 | 214 (84.6) |
| ≥ 115 | 39 (15.4) |
| Missing | 2 |
| Stimulated TG ABS (IU/mL) | 18 (15–46) |
| < 115 | 213 (87.3) |
| ≥ 115 | 31 (12.7) |
| Missing | 11 |
Therapeutic interventions and response assessment
Most patients underwent initial thyroidectomy at Sultan Qaboos University Hospital (47.1%) or Armed Forces Hospital (18.8%). Lymph node dissection was performed in 40.0% of cases.
Neck ultrasound conducted post-surgery revealed no residual findings in 78.1% of patients, while lymphadenopathy and residual thyroid tissue were seen in 13.7% and 8.2%, respectively. Postoperative whole-body scans indicated uptake limited to the neck in 89.4% of cases. Lymph node and distant uptake were observed in 5.5% and 5.1%, respectively.
Most patients (87.1%) received a single dose of radioactive iodine (RAI), with a median cumulative dose of 3.7 mCi (range: 1.1–23.3). Only 2.3% of patients required external beam radiotherapy, and 7.8% underwent a second surgical intervention, primarily for lymph node dissection.
At six months post-treatment, 71.3% of patients had a TG level < 0.2 ng/mL. This increased slightly to 73.3% by the last follow-up. TG-Abs remained negative (< 115 IU/mL) in over 91% of patients at both time points (Table 5, Figure 3).
Table 5. Outcomes post- surgery and radio-active iodine in differentiated thyroid cancer patients.| Response Parameters | Median (IQR) or n (%) (unless defined otherwise) |
|---|---|
| Place of surgery | |
| SQUH | 120 (47.1) |
| AFH | 48 (18.8) |
| SQCCCRC | 25 (9.8) |
| Other government hospitals | 23 (9.0) |
| Private hospitals | 17 (6.7) |
| Abroad | 22 (8.6) |
| LN dissection | |
| Yes | 102 (40.0) |
| No | 153 (60.0) |
| US post-surgery | |
| Negative | 199 (78.1) |
| Lymphadenopathy | 35 (13.7) |
| Residual thyroid tissue | 21 (8.2) |
| WBS post-surgery | |
| Neck uptake only | 228 (89.4) |
| Positive lymph nodes | 14 (5.5) |
| Distant metastasis | 13 (5.1) |
| Number of RAI doses | |
| 1 | 222 (87.1) |
| 2 | 21 (8.2) |
| 3 | 9 (3.5) |
| 4 | 2 (0.8) |
| 5 | 1 (0.4) |
| TG at 6 months (ng/mL) | 0.04 (0.04–0.31) |
| < 0.2 | 179 (71.3) |
| ≥ 0.2 | 72 (28.7) |
| Missing | 4 |
| TG Antibodies at 6 months (IU/mL) | 15 (18–27) |
| < 115 | 230 (91.6) |
| ≥ 115 | 21 (8.4) |
| Missing | 4 |
| TG at last follow-up (ng/mL) | 0.04 (0.04–0.24) |
| < 0.2 | 184 (73.3) |
| ≥ 0.2 | 67 (26.7) |
| Missing | 4 |
| TG Antibodies at last follow-up (IU/mL) | 18 (17–24) |
| < 115 | 237 (94.4) |
| ≥ 115 | 14 (5.6) |
| Missing | 4 |
| Cumulative dose given ( mCi ) (range) | 3.7 (1.1–3.7) (1.1–23.3) |
| Radiation therapy | |
| Yes | 6 (2.3) |
| No | 249 (97.7) |
| Second surgery | |
| Yes | 20 (7.8) |
| – LN dissection only | 19 (95) |
| – Removal of skull and brain metastasis | 1 (5) |
| No | 235 (92.2) |
Figure 3. Place of Surgery in or outside Sultanate of Oman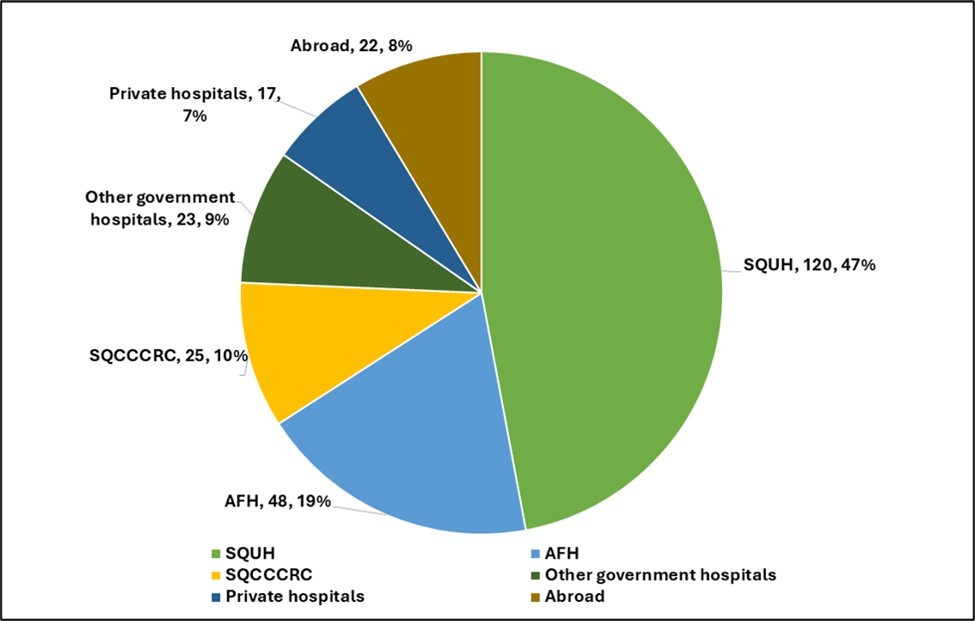
Download figure
Predictors of therapeutic response at 6 months and at last follow-up
We evaluated predictors of biochemical response (defined as TG < 0.2 ng/mL) at two key time points: 6 months post-RAI therapy and at the last follow-up.
At 6 months post-RAI, several variables were significantly associated with achieving a disease-free state. These included female sex (p = 0.006), absence of lymph node involvement (p = 0.001), no distant metastasis (p < 0.001), absence of extrathyroidal extension (p < 0.001), and lack of angio-vascular invasion (p < 0.001). Tumor size was also associated with early response, with T1 tumors showing better outcomes than T2–T4 tumors (p = 0.011). Patients classified as AJCC stage I or ATA low-risk had significantly higher rates of early response (p < 0.001 for both). While younger age (<45 years) appeared favorable, it only approached statistical significance (p = 0.050).
At last follow-up, the associations remained largely consistent. Female sex (p = 0.004), T1 tumor size (p = 0.032), absence of lymph node involvement (p = 0.003), absence of distant metastasis (p < 0.001), lack of extrathyroidal extension (p < 0.001), and absence of angio-vascular invasion (p = 0.003) continued to predict favorable response. Age <45 years achieved significance (p = 0.032). Notably, both age and tumor size, when treated as continuous variables, were not significantly associated with TG response at either time point (age: p = 0.325 at 6 months, p = 0.411 at last follow-up; tumor size: p = 0.107 at 6 months, p = 0.232 at last follow-up), suggesting a potential non-linear relationship.
Risk stratification continued to be predictive at both time points: patients with ATA low-risk disease were significantly more likely to achieve TG < 0.2 ng/mL at 6 months (85% vs. 33% in high-risk group; p < 0.001) and at last follow-up (85% vs. 40%; p < 0.001). Similarly, AJCC stage I was strongly associated with better outcomes (p < 0.001).
Follow-up duration also played a role. At 6 months, patients followed for ≤12 months had higher rates of biochemical response (p = 0.004), and this association remained significant at last follow-up (p < 0.001), although it may partially reflect lead-time bias.
In the multivariable logistic regression model for response at 6 months, tumor size (T1) was significantly associated with a favorable response, with patients having T1 tumors more likely to achieve TG < 0.2 ng/mL (p = 0.039; OR = 0.462, 95% CI: 0.222–0.963).
The presence of distant metastasis was excluded from the model due to perfect separation: all patients with distant metastasis had persistent disease, while none of the patients without metastasis achieved persistent disease. As a result, this variable was omitted due to perfect prediction and collinearity. At the last follow-up, the presence of distant metastasis remained a statistically significant independent predictor of persistent disease (p = 0.006; OR = 0.02, 95% CI: 0.001–0.315). Additionally, follow-up duration >12 months was independently associated with persistent disease at this time point (p = 0.039; OR = 0.404, 95% CI: 0.171–0.954) (Table 6, Figure 4).
Table 6. Predictors of outcomes in differentiated thyroid cancer patients.| Variables | Outcomes at 6 months post RAI, Percentage or mean ± SD | P-value | Outcomes at last follow-up, Percentage or mean ± SD | P-value | ||
| Disease-free (TG <0.2 ng/mL) | Persistent disease (TG ≥0.2 ng/mL) | Disease-free (TG <0.2 ng/mL) | Persistent disease (TG ≥0.2 ng/mL) | |||
| Age (years) | 39.2 ± 11.0 | 40.9 ± 15.1 | 0.325 | 39.3 ± 11.0 | 40.8 ± 14.6 | 0.411 |
| < 45 years | 75 | 25 | 0.050 | 77 | 23 | 0.032 |
| ≥45 years | 63 | 37 | 64 | 36 | ||
| Sex | ||||||
| Female | 76 | 24 | 0.006 | 78 | 22 | 0.004 |
| Male | 56 | 44 | 58 | 42 | ||
| BMI (kg/m ² ) | 30.3 ± 6.4 | 30.2 ± 6.4 | 0.977 | 29.8 ± 6.2 | 31.4 ± 6.8 | 0.113 |
| < 30 | 73 | 27 | 0.317 | 77 | 23 | 0.120 |
| ≥ 30 | 69 | 31 | 69 | 31 | ||
| Histopathological subtype | ||||||
| Papillary | 71 | 29 | 0.410 | 75 | 25 | 1.000 |
| Non-papillary | 82 | 18 | 80 | 20 | ||
| Tumor size | 2.2 ± 1.5 | 2.6 ± 2.1 | 0.107 | 2.2 ± 1.5 | 2.5 ± 1.9 | 0.232 |
| T1 | 80 | 20 | 0.011 | 81 | 19 | 0.032 |
| T2–T4 | 66 | 34 | 69 | 31 | ||
| LN status | ||||||
| N0 or Nx | 81 | 19 | 0.001 | 82 | 18 | 0.003 |
| N1 | 62 | 38 | 65 | 35 | ||
| Metastasis | ||||||
| M0 | 78 | 22 | <0.0001 | 79 | 21 | <0.0001 |
| M1 | 0 | 100 | 9.1 | 90.9 | ||
| Extrathyroidal extension | ||||||
| No | 78 | 22 | <0.0001 | 80 | 20 | <0.0001 |
| Yes | 36 | 64 | 39 | 61 | ||
| Angio-vascular invasion | ||||||
| No | 81 | 19 | <0.0001 | 81 | 19 | 0.003 |
| Yes | 59 | 41 | 63 | 37 | ||
| Tumor focality | ||||||
| Unifocal | 74 | 26 | 0.915 | 77 | 23 | 0.095 |
| Multifocal | 73 | 27 | 75 | 25 | ||
| AJCC stage | ||||||
| Stage I | 78 | 22 | <0.0001 | 79 | 21 | <0.0001 |
| Stage II–IV | 26 | 73 | 33 | 67 | ||
| ATA risk score | ||||||
| Low | 85 | 15 | <0.0001 | 85 | 15 | <0.0001 |
| Intermediate | 68 | 32 | 71 | 29 | ||
| High | 33 | 67 | 40 | 60 | ||
| Duration of follow-up (months) | 16.2 ± 13.3 | 22.5 ± 17.4 | 0.004 | 18.2 ± 18.8 | 31.7 ± 21.9 | <0.0001 |
| ≤12 months | 82 | 18 | 0.067 | 86 | 14 | 0.018 |
| >12 months | 71 | 29 | 72 | 28 | ||
Figure 4. Outcomes at last follow-up, percentage of disease-free (TG <0.2 ng/mL)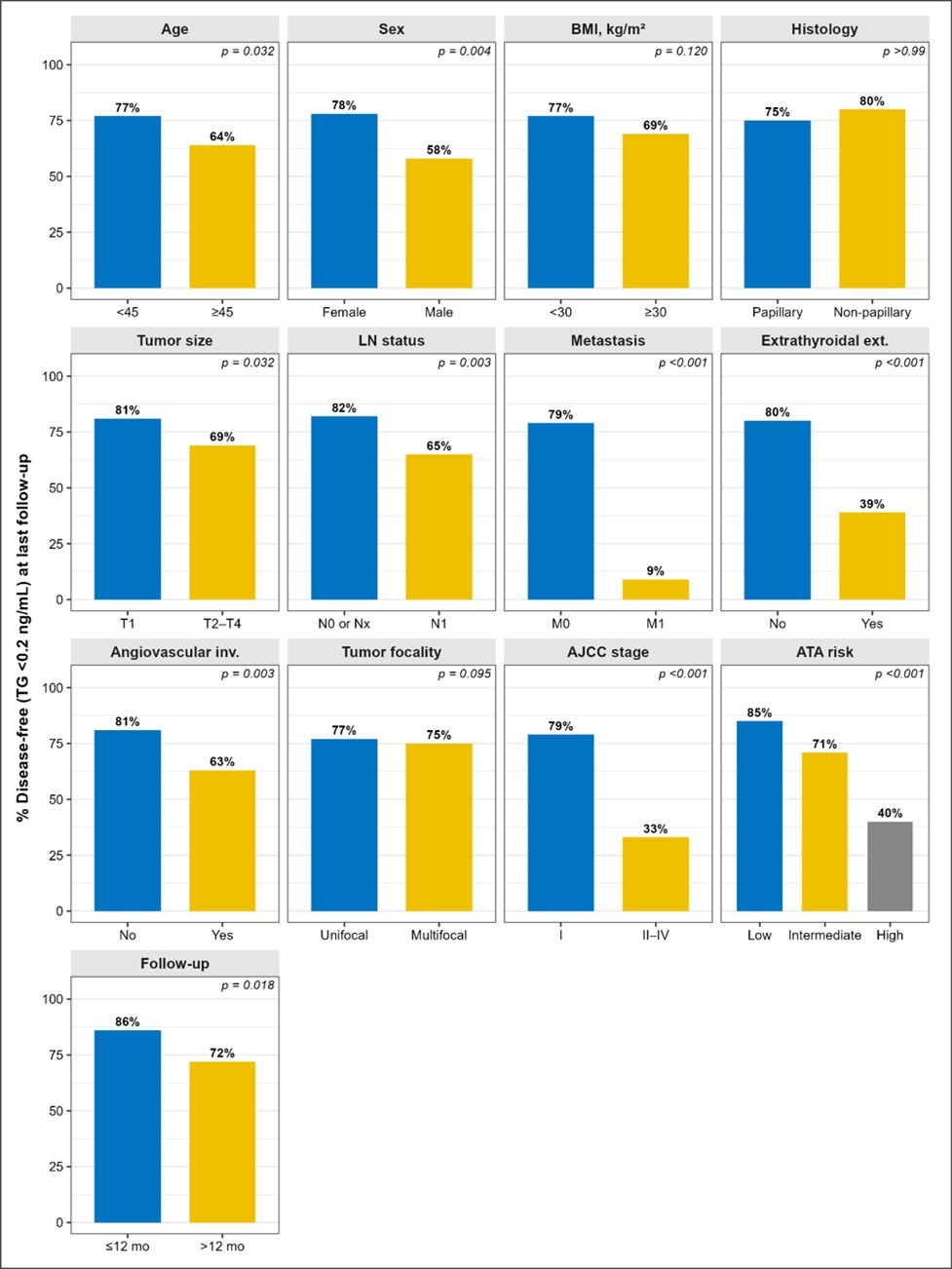
Download figure
Discussion
Well differentiated thyroid cancer, the second most diagnosed cancer in Oman 3, largely has a favourable prognosis. Surgery and radioiodine therapy are the two pillars of differentiated thyroid ca therapy especially in the setting of curative intent. Long term TSH suppression, radiotherapy, tyrosine kinase inhibitors and redifferentiation therapies are additional options to achieve disease control when cure can’t b be achieved. This study looks at the relationship between patient and disease factors in 255 patients managed at SQCCCRC with surgery and radioiodine and outcome of therapy at 6 months and at last follow up which was a median of 14 months.
Excellent response defined in this study as non-stimulated Tg < 0.2ng/ml, was seen in 72.1% of our patients at last follow up. This is much less than 82.7% disease free survival previously reported in the Omani population 13. This discrepancy is likely due to longer follow up and additional treatment to achieve disease free status in the prior study.
The percentage of patients with non-stimulated Tg < 0.2ng/ml post operatively was 34%. This increased to 70% at 6 months post radioactive iodine. Multiple factors that correlate with low-risk disease predicted this excellent response. These are T1 tumours, female gender, absence of lympho-vascular invasion, absence of extrathyroidal extension and absence of distant metastasis. Multivariate analyses however showed tumour size as a significant predictor of response with T1 tumours being more likely to achieve excellent response. None of the cases with distant metastases achieved excellent response during the follow up period. ATA low risk and AJCC stage 1 disease unsurprisingly are significantly associated with excellent response.
The age and gender distribution in our patient population is comparable to prior study in Oman 13. There is an overwhelming female preponderance with most presenting in the fourth decade. The age of peak incidence is similar to Saudi Arabia 14 but our patients tend to be younger compared to Australia, UK and US 15. The younger age of incidence is not attributable to incidental diagnosis as there is no routine screening program. Both age less <45 years and female gender have strong association with excellent response. This finding is similar to many prior studies 16, 17, 18 but differ from prior study in Oman 13. This may be related to the follow up duration which was longer in the Oman study and measured outcome – disease free survival vs excellent response.
There is a strong association between tumour size <1cm and excellent response as previously reported in multiple studies 17, 19. No separate analysis of patients with tumours ≥4cm was done due to limited number of patients. In our patient population, about half of the patients were obese but more importantly, all patients with AJCC stage 4 disease were obese. These patients are only 3% of our study cohort and we are unable to draw a definite association between obesity and advanced stage disease.
A very important finding in our study is the distribution of advanced disease based on the region of Oman the patient is referred from. The highest proportion of patients are from the Al-Batinah province, followed by Muscat mirroring the higher population of these governorates. The Dhofar governorate had majority (38%) of the cases with distant metastases while only having 9% of total cases. About one out of four patients referred from the Dhofar province had distant metastases and this was statistically significant. Possible explanation of the latent is late diagnosis because of societal behaviour that favours delay in seeking treatment. In addition, there may be underlying biological or genetic differences associated with more aggressive disease behavior in this population, although this would require further investigation. A higher prevalence of obesity in Dhofar may also contribute to more advanced disease at presentation 20.
Significant number of patients in our cohort are ATA low risk – 45.9%. These patients had total thyroidectomy and radioactive iodine which is not entirely in line with current trend of a more conservative approach to treatment 16. These warrants further protocol and multidisciplinary review to ensure a balance between over and under treatment. Monitoring those patients for recurrence with thyroglobulin will however be much easier following complete ablation of the thyroid. One possible explanation is the logistical challenge of long-term surveillance. Conservative management requires strict and close follow-up, including serial imaging and biochemical monitoring. In settings where access to care, geographic distance, or patient compliance may be suboptimal, maintaining such surveillance can be difficult and may increase the risk of loss to follow-up. In contrast, total thyroidectomy with radioactive iodine facilitates simpler and more reliable monitoring through serum thyroglobulin, potentially making follow-up more practical in this context.
Our experience in low-risk patients is that a good proportion have rising tg levels within few years, as well some develop cervical lymph nodes and lung metastasis. Recently one patient with NIFT-P, which is classified as very low risk, post total thyroidectomy, his Tg levels increased and doubled from 9 to 18 ug/L in 6 months period post-surgery.
These cases and more are the reasons why we give ablative dose even to low-risk patients especially when they have some features that may push them to intermediate risk. We cautiously follow the guidelines in these cases and having as well-designed randomised controlled trial in low and low to intermediate risk patients will go a long way in establishing best practices in our region.
Our findings on disease outcome at median of 14 months follow up is consistent with prior research on favourable outcome in differentiated thyroid ca. Other than the retrospective nature of this study, another limitation of the study is short follow up time as disease recurrence is known to occur for up to 10 years after initial treatment.
Conclusion
The outcome of therapy in majority of our patients is favourable with 72% having excellent biochemical response at last follow up. With none of our patients with distant metastasis achieving excellent response and a high proportion of them coming from the Dhofar governorate, a targeted intervention would be of benefit. Late diagnosis due to poor health care seeking behaviour is a possible major contributor which can be addressed with focussed health education.
Low risk patients warrant study, very close follow up and further protocol and multidisciplinary review to establish the best practices in our region
References
- 1.Sung H, Ferlay J, Siegel R L, Laversanne M, Soerjomataram I et al. (2021) . Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer 71(3), 209-49.
- 2.Al-Lawati N A, Al-Bahrani B J, Al-Raisi S S, Al-Lawati J A. (1996) Twenty-year trends of cancer incidence in Omanis. Oman Med 34(4), 361-87.
- 3.Al-Lawati N A, Shenoy S M, Al-Bahrani B J, Al-Lawati J A. (2020) Increasing Thyroid Cancer Incidence in Oman: A Joinpoint Trend Analysis. Oman Med J.
- 4. (2019) Department of Non-Communicable Diseases. 20 years cancer incidence in Oman report (1996-2015) [Internet]. Ministry of Health.
- 5. (2022) Department of Non-Communicable Diseases. Cancer Incidence in. [Internet]. Ministry of Health , Oman
- 6.Iwasaki H, Yamazaki H, Takasaki H, Suganuma N, Sakai R et al. (2019) Treatment outcomes of differentiated thyroid cancer with distant metastasis improve by tyrosine kinase inhibitors. , Oncology letters 17(6), 5292-5300.
- 7.Kunadharaju R, Goyal G, Rudraraju A, P T Silberstein. (2015) New Treatment Options for Metastatic Thyroid Cancer. Federalpractitioner :for the health care professionals of the VA, DoD, and PHS. 32, 21-26.
- 8.Lortet-Tieulent J, Franceschi S, Dal Maso L, Vaccarella S. (2019) Thyroid cancer “epidemic” also occurs in low- and middle-income countries. , Int 144(9), 2082-7.
- 10.Konishi T, Fujiogi M, Michihata N, Niwa T, Morita K et al. (2021) Impact of body mass index on short-term outcomes after differentiated thyroid cancer surgery: a nationwide inpatient database study in Japan.Eur Thyroid J. 11-1.
- 11.Papachristos A J, Nicholls L E, Mechera R, Aniss A M, Robinson B et al. (2023) Management of Medullary Thyroid Cancer: Patterns of Recurrence and Outcomes of Reoperative Surgery. The Oncologist. 232.
- 12.Rahman G A. (2011) Extent of surgery for differentiated thyroid cancer: recommended guideline. Oman Med J. 26-1.
- 13.Kunjumohamed F P, Al Rawahi A, Al Busaidi NB, Al Musalhi HN. (2021) Disease-free Survival of Patients with Differentiated Thyroid Cancer: A Study from a Tertiary Center in Oman.Oman Med J. 36-2.
- 14.Flemban A, Kabrah S, Alahmadi H, Alqurashi R, Turaes A et al. (2022) . Patterns of Thyroid Cancer Mortality and Incidence in Saudi Arabia: A 30-Year Study. Diagnostics 12(11), 2716.
- 15.Weller S, Chu C, Lam AK yin. (2025) Assessing the Rise in Papillary Thyroid Cancer Incidence: A 38-Year Australian Study Investigating WHO Classification Influence. J Epidemiol Glob Health. 15(1), 9.
- 16.Robertson B, Parker M, Shepherd l, Panieri E, Cairncross l et al. (2018) Nodal disease predicts recurrence whereas other traditional factors affect survival in a cohort of South African patients with differentiated thyroid carcinoma. Cancers Head Neck. 3(1), 10.
- 17.Hajj Boutros r, Arabi A, Shoucair M, Abbas J, Salti I. (2018) Disease free survival of well differentiated thyroid cancer: 20 years’ experience at a tertiary care center in Lebanon. Int Arch Med. 11, 2545.
- 18.Mallick U, Newbold K, Beasley M, Garcez K, Wadsley J et al. (2025) Thyroidectomy with or without postoperative radioiodine for patients with low-risk differentiated thyroid cancer in the UK (IoN): a randomised, multicentre, non-inferiority trial. The Lancet. 406(10498), 52-62.